
Prophylactic Mastectomy & Reconstruction in Mumbai
Prophylactic Mastectomy & Reconstruction
A Difficult Decision, Made With Full Information and Care
If you are a BRCA1 or BRCA2 mutation carrier, or carry another high-risk gene mutation, you live with a lifetime breast cancer risk significantly higher than the general population up to 70% for BRCA1 carriers, depending on family history and age. The same is true for women with multiple close relatives diagnosed with breast cancer at a young age. Risk-reducing (prophylactic) mastectomy with immediate reconstruction is one of the most effective preventive options available reducing breast cancer risk by approximately 90–95%.
This is not a decision to be made quickly, alone, or without expert support. Dr. Rachana Tataria provides comprehensive prophylactic mastectomy and reconstruction in Mumbai at Fortis Hospital, Mulund, alongside breast oncology and genetic counselling colleagues. With an FRCS in Plastic Surgery from the Royal College of Surgeons, England, and dual fellowships in oncoplastic breast surgery and breast microvascular reconstruction at UK NHS hospitals, she brings the experience of a high-volume international centre to high-risk patients in India including a deep understanding of the emotional weight of this surgery, particularly for younger women still considering future children.
Who Should Consider Prophylactic Mastectomy?
Women confirmed as BRCA1 or BRCA2 mutation carriers through genetic testing.
Women with TP53, PALB2, or other high-penetrance gene mutations.
Women with a strong family history of breast cancer (multiple first-degree relatives, early-age diagnoses, bilateral disease, or male breast cancer in the family).
Women diagnosed with breast cancer in one breast who are at high risk in the other (contralateral prophylactic mastectomy).
Women previously treated with chest wall radiotherapy in childhood (e.g. for Hodgkin lymphoma).
Women whose surveillance with MRI and mammography has caused significant ongoing anxiety or repeated suspicious findings.
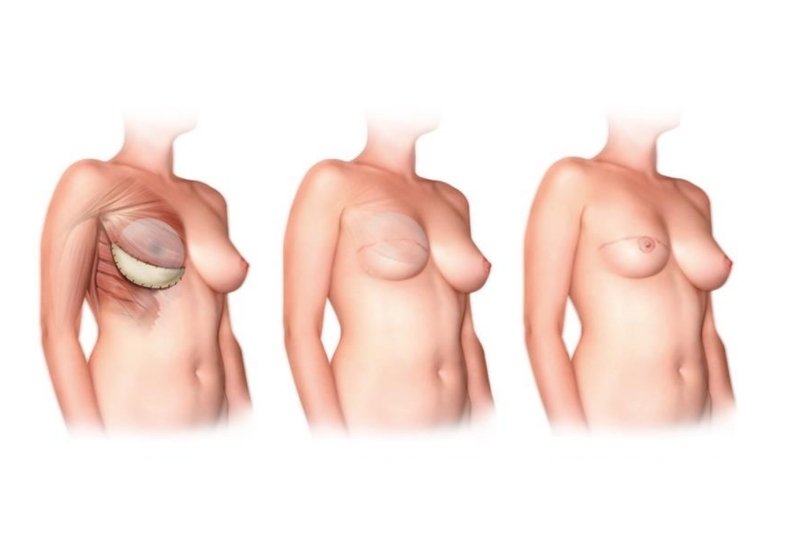
Types of Prophylactic Mastectomy Offered

Nipple-Sparing Mastectomy (NSM)
Preserves the entire skin envelope and the nipple-areola complex, removing only breast tissue underneath
Skin-Sparing Mastectomy (SSM)
Preserves the breast skin but removes the nipple-areola complex. Used when nipple preservation is not appropriate.
Total Mastectomy with Reconstruction
Removes all breast tissue and the nipple, with reconstruction performed at the same operation.
Why Choose LD Flap Reconstruction?
Bilateral cases offer an excellent opportunity for symmetric, natural-appearing reconstruction because both breasts are reconstructed together often producing better symmetry than single-side reconstruction after cancer surgery. In almost all prophylactic cases, immediate breast reconstruction is performed during the same operation, so the patient never wakes up without a breast mound. Reconstruction options include:
Direct-to-Implant (DTI) Reconstruction
Particularly suited to women undergoing bilateral risk-reducing mastectomy.
Two-Stage Tissue Expander
Two-Stage Tissue Expander to Implant reconstruction.
DIEP flap, TUG flap, or LD flap
Natural-tissue reconstruction options chosen based on body type and patient preference.
Why Choose Dr. Rachana Tataria for Prophylactic Mastectomy in Mumbai
01
Experience with bilateral nipple-sparing mastectomy and immediate reconstruction during UK NHS practice at Wythenshawe Hospital, Manchester and University Hospital Coventry & Warwickshire.
02
FRCS Plastic Surgery, Royal College of Surgeons, England rare international credentials in Mumbai.
03
Coordination with breast oncologists, genetic counsellors, and psycho-oncology support at Fortis Hospital, Mulund.

04
Female plastic surgeon many BRCA patients prefer this for a deeply personal preventive surgery, especially when considered alongside future fertility, pregnancy, and breastfeeding decisions.
05
Confidential, unhurried consultations decisions about prophylactic surgery should never be rushed.
06
Multilingual consultation: English, Hindi, Marathi, Gujarati, Kutchi, Kannada, and French.
The Patient Pathway
Full discussion of risk, options, and timing. No decision is made in a single visit.
Genetic counselling and confirmatory testing (if not already done).
Breast oncology, plastic surgery, genetic counselling, and (where needed) psycho-oncology input.
Recent MRI, mammogram, and ultrasound.
Choice of implant-based or autologous flap reconstruction, with detailed counselling on each.
Surgery and immediate reconstruction at Fortis Hospital, Mulund.
Including long-term breast health monitoring of any residual tissue.
The Recovery Journey
Recovery Based on Reconstruction Type
Recovery timelines vary depending on whether implant-based or flap-based reconstruction is performed.
Shorter Recovery with Implant Reconstruction
Implant-based procedures usually involve a 1–2 night hospital stay and quicker return to work.
Drain Removal and Healing Support
Drains are typically removed within 1–2 weeks as healing progresses after the surgery.
Emotional Care and Follow-Up Support
Ongoing follow-up appointments and psycho-oncology support help patients through emotional recovery.
FAQs : Prophylactic Mastectomy in Mumbai
Prophylactic bilateral mastectomy reduces breast cancer risk by approximately 90–95% in BRCA mutation carriers and women with similar high-risk profiles. Risk is reduced but not eliminated, as a small amount of breast tissue can remain.
No. Prophylactic mastectomy removes the breast tissue including milk-producing glands, so breastfeeding is not possible afterwards. For women planning future children, the timing of surgery in relation to family planning is a major part of consultation.
Yes, sensation is usually significantly reduced or lost, including erotic sensation. Some return of light touch sensation can occur over 1–2 years in some patients, but this is variable.
Most guidelines suggest considering surgery from age 25–30 onwards for BRCA1 carriers and slightly later for BRCA2, but timing is highly individualised based on family history, personal preference, and life stage.
Coverage varies. Many policies cover prophylactic mastectomy and reconstruction for confirmed high-risk gene carriers with documented oncology recommendation, but pre-authorisation is essential and is handled by the clinic team.
Routine mammography is no longer needed after prophylactic mastectomy, but periodic clinical examination is recommended to check the chest wall and any residual tissue. Other cancer screenings (ovarian for BRCA carriers) continue.
Bilateral nipple-sparing mastectomy with implant reconstruction typically takes 4–6 hours. With flap reconstruction (such as bilateral DIEP), it can take 10–14 hours and involves a microsurgical team.
Get in Touch with Dr. Rachana Tataria
Whether you’re ready to take the next step or have questions about Prophylactic Mastectomy, we are here to guide you.
Begin your journey toward transformation.